From the very beginning, Dr. Richard Pinson and I have taught hospitals that coding specialists, not just nurses, can and should perform the CDI function. We have always included coders in our training sessions and advised hospitals to consider coders for the CDI role. Just as CDI specialists benefit from learning coding guidelines and principles, coding specialists can and should learn the clinical criteria.
As an employer, you may benefit from a team approach with both CDI specialists and coding professionals who are able to identify documentation issues that will result in meaningful changes to the ultimate codes and reimbursement. Making the most of both areas of expertise results in a more efficient and productive CDI function.
How can a coder be an effective part of the CDI function?
For coders, enhancing their understanding of diagnostic criteria and the disease processes will give them the ability to see all clinical relationships pertinent to the patient’s conditions.
More knowledge of these diagnostic criteria and disease processes will give coders more confidence as an equal partner in the CDI team and able to provide their non-coding colleagues with additional insight to the intricacies and challenges of the coding systems.
More clinical knowledge will alert coders to the need for queries when the documentation is lacking and will help the coder to prepare a more appropriate and effective provider query.
As a final benefit, coders with a firm grasp of the diagnostic criteria and disease processes may decide to take the leap and advance their career as a CDI specialist.
When we first created the CDI Pocket Guide®15 years ago, CDI was an emerging field and there was no reference tool available. Hospitals had to hire an expensive consulting firm, and even then, the educational materials were large three-ring binders containing hundreds of pages of information that was virtually impossible to reference and often the coders were left out.
The CDI Pocket Guide® was written with both coding and CDI professionals in mind. It offers coding and CDI specialists the tool they need to quickly and easily access the clinical definitions, diagnostic criteria, treatment considerations and specific challenges for the key clinical conditions encountered in the hospital. The CDI Pocket Guide® has become the most highly respected unofficial source for authoritative CDI information. Thousands of coders and CDS have come to rely on it, often telling us it’s their “CDI bible.”
Get our CDI Pocket Guide® and access our informative webinars on important coding and CDI topics.
MCC-CC Listings for MS-DRGs FY2022
Complete MCC and CC Listings for FY2022 beginning October 1, 2021. Also includes the additions and deletions to the MCC and CC lists for FY2022.
Myocardial Ischemia, Myocardial Injury and Myocardial Infarction
Would you please explain the basics of the process from myocardial ischemia to injury to infarct? At what point does injury become an infarct?
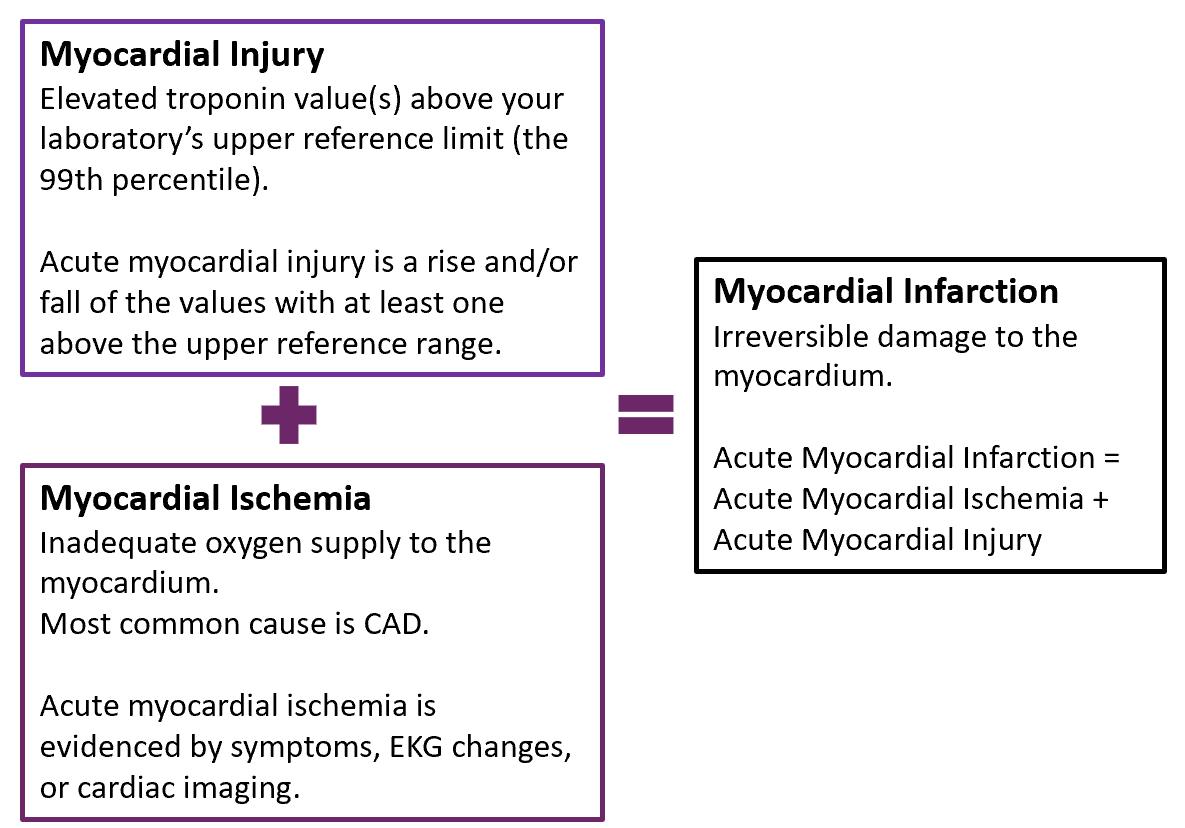
We'll start by defining myocardial ischemia, injury and infarction.
Myocardial ischemia simply means there is inadequate oxygen supply to the myocardium without damage to myocardial cells. No troponin is released in patients with chronic ischemia. The most common cause of ischemia is coronary artery disease (CAD). Patients who have CAD have chronically reduced oxygen supply to the myocardium putting them at risk for acute ischemia when oxygen demand exceeds oxygen supply, for example, when a person with CAD over-exerts causing angina.
Acute myocardial ischemia is evidenced by symptoms, EKG changes or cardiac imaging. If troponin is also released and above the 99th percentile (i.e., acute myocardial injury), a myocardial infarction has occurred. If not, then the patient only has unstable angina or demand ischemia.
Get our CDI Pocket Guide® to learn more about myocardial injury, ischemia, and infarction.
Myocardial injury is considered acute when there is a rise and/or fall of troponin values, with at least one above the 99th percentile. When chronic, the troponin levels remain stable at a constantly elevated level. Myocardial injury may be due to ischemic or nonischemic causes.
To diagnose a myocardial infarction, the patient must have acute myocardial injury as well as evidence of acute myocardial ischemia (symptoms, EKG findings, imaging evidence).
Myocardial injury (acute or chronic) without evidence of acute myocardial ischemia is a non-MI troponin elevation secondary to a non-ischemic cause, i.e., non-ischemic myocardial injury. As of October 1, 2021, there is a new ICD-10 code I5A to capture the diagnosis of non-ischemic myocardial injury.
Myocardial Infarction is irreversible ischemic “injury” to the myocardium. An acute myocardial infarction occurs when acute myocardial ischemia causes myocardial injury. In other words, acute myocardial injury + acute myocardial ischemia = acute myocardial infarction.
Further details regarding evidence of acute myocardial ischemia, elevated troponin levels (myocardial injury), and ischemic vs. non-ischemic causes of myocardial injury are provided below.
Acute Myocardial Ischemia
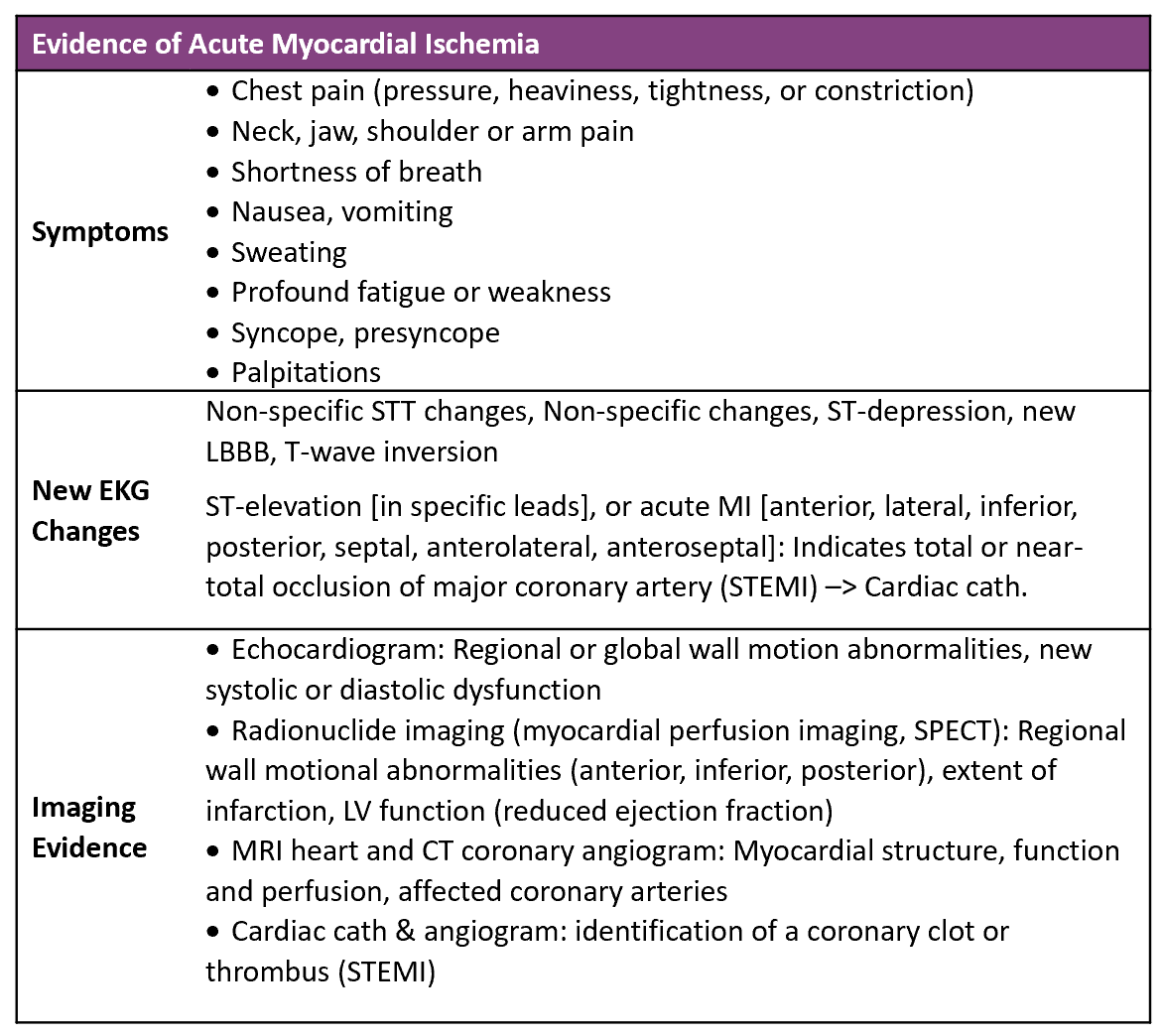
For a diagnosis of acute myocardial infarction there must be evidence of acute myocardial ischemia. There are three ways you could look for evidence of myocardial ischemia: (1) symptoms, (2) new EKG changes and (3) imaging evidence.
Evidence of Acute Myocardial Ischemia
Symptoms. The symptoms of ischemia are also those that are often consistent with an acute coronary syndrome or myocardial infarction. But they're not just chest pain, pressure, heaviness, tightness. There are many things that may be associated with myocardial ischemia that we may not think of. Most of us are familiar with the chest pain with radiation to neck, jaw, shoulder or arm, which is usually on the left side. Sometimes there's an epigastric location, but that may be difficult to separate from the substernal location and may accompany it. Shortness of breath, nausea, vomiting, sweating are not unusual. Some people only express a sense of profound fatigue or weakness. Syncope or presyncope can be the only symptom, and that's usually due to some type of an arrhythmia associated with an ischemic myocardium.
New EKG changes. The above table is intended to list things you may actually see on the EKG report or that may be described by the physicians when they're talking about the EKG and evidence of ischemia such as nonspecific STT changes, or nonspecific STT-wave changes, or “nonspecific changes”, or ST-depression, or new left bundle branch block, new Q-waves, or T-wave inversion
ST elevation is characteristic of STEMI and the EKG may say ST elevation in certain specific leads, like leads 2,3 and aVF, or 1 and aVL or V1-V3. Alternatively, the location of the MI may be stated like inferior, lateral or anterior.
Cardiac Imaging. Imaging evidence includes echocardiogram, the radioactive nuclide imaging (myocardial perfusion), or SPECT. MRI of the heart and CT angiograms, or cardiac cath with angiography, and other modalities can identify wall motion abnormalities, systolic or diastolic dysfunction, changes in ejection fraction. Extent of infarct is sometimes identified as well as structural abnormalities, perfusion abnormalities of affected coronary arteries and with cardiac cath intracoronary thrombus may be identified.
Elevated Troponin Levels: Myocardial Injury
Troponin levels in suspected myocardial infarction are measured on admission, typically two to four hours after admission, six to eight hours after admission for the third, and occasionally a fourth measurement at 12 hours depending on whether the first three are diagnostic or not. Troponin I is preferred to troponin T because it's a little more specific and a bit more accurate.
In general, higher troponin levels are associated with more extensive myocardial injury. Peak troponin values are usually highest in STEMIs, then NSTEMIs, and lowest overall in non-ischemic (non-MI) causes. Keep in mind though that a very high troponin level alone is not diagnostic of a myocardial infarction and must be supported by evidence of acute myocardial ischemia.
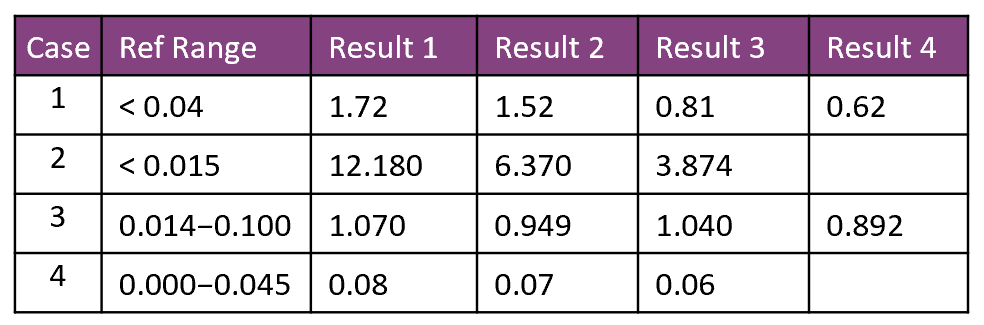
Elevated Troponin Levels
In Case #1, there is evidence of acute myocardial injury because the troponin level is very high compared to the URL of 0.04 and it falls from 1.72 to 0.62. If there is also evidence of acute myocardial ischemia (symptoms, new EKG changes, cardiac imaging), we have an acute myocardial infarction either Type 1 or Type 2, depending on the cause.
The same is true for Case #2 where there is a dramatic fall from a very high level of 12.180 to 3.874, compared to the upper reference limit of 0.015. Elevated troponin levels of this magnitude are often associated with a STEMI.
In Case #3, the troponin level is elevated but there is a slight fall and then a slight rise occurs followed by another fall that is more or less stable without a clear trend. This likely represents chronic nonischemic myocardial injury.
Case #4 shows only very slightly elevated levels and are rather flat. We don't really know if they are dropping. These might be within the normal range for this patient even though these are above the normal reference range.
How quickly does the troponin level disappear after injury? It can take up to two weeks for the troponin level to return to normal, so a delayed diagnosis of myocardial infarction can still be made.
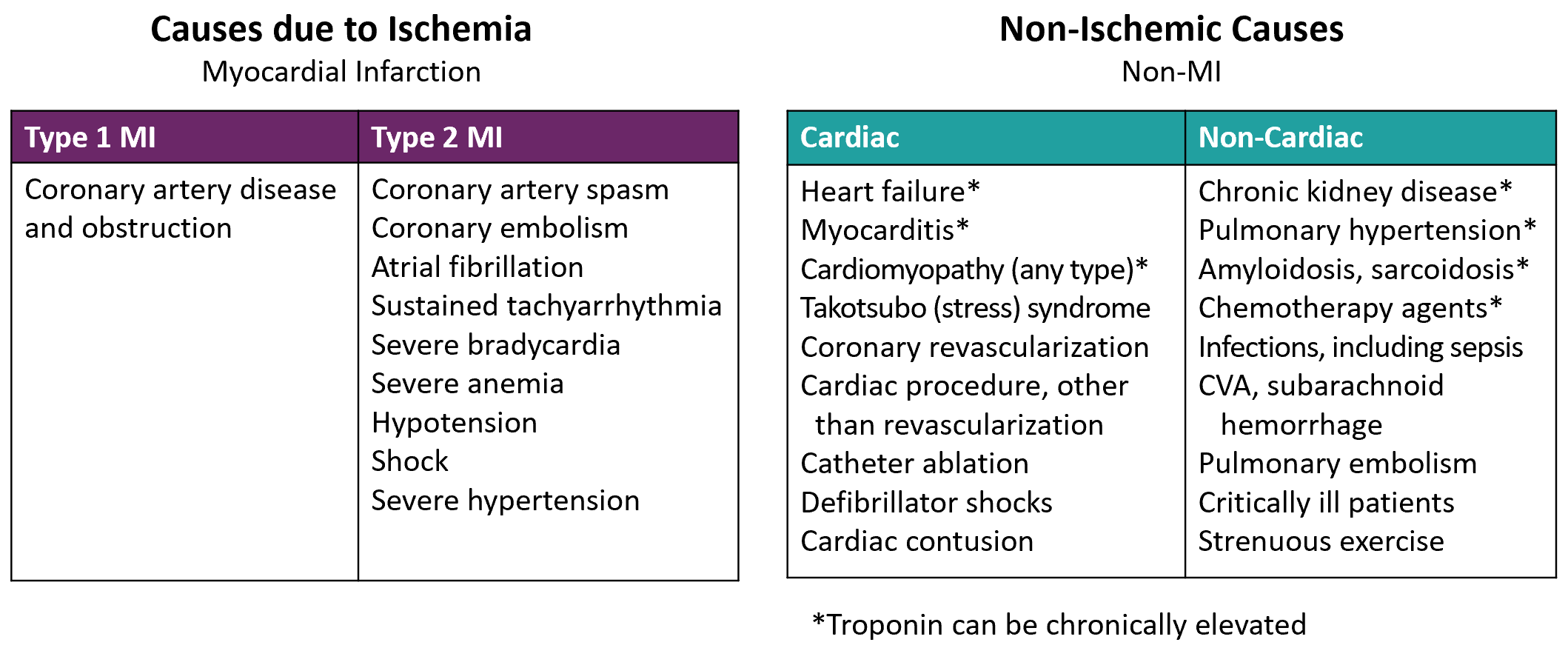
Causes of Elevated Troponin Levels: Myocardial Injury
The above table shows the ischemic and other nonischemic causes of myocardial injury. Ischemic causes of myocardial injury in the setting of acute myocardial ischemia are myocardial infarctions of all types, most commonly Types 1 and 2. The causes of Type 2 MI are non-CAD causes and included above.
If the cause of the myocardial injury is non-ischemic, there is no myocardial infarction. It's important to recognize that patients with heart failure, cardiac procedures, infections, critical illness, kidney disease, CVA and many other noncoronary causes can have elevated troponin levels, but without an ischemic cause, there is no myocardial infarction. Do not query for a myocardial infarction unless there is evidence of acute myocardial ischemia.
This is not to say that patients with these conditions cannot also have acute myocardial ischemia, such as the patient with both heart failure and CAD. Do not query for a myocardial infarction unless there is evidence of acute myocardial ischemia.
Summary: Myocardial Injury, Myocardial Ischemia and Myocardial Infarction
Myocardial injury is defined as an elevation of cardiac troponin values with at least one value above the 99th percentile upper reference limit. Acute myocardial injury is when there is a rise and/or fall of the troponin levels. Myocardial injury can be either acute or chronic and due to ischemic (CAD) or non-ischemic causes.
There are multiple causes of nonischemic myocardial injury that are both cardiac and noncardiac. A new ICD-10 code I5A has been created for non-ischemic myocardial injury.
Acute myocardial ischemia is identified by symptoms, new EKG changes, and/or cardiac imaging.
Acute myocardial infarction (AMI) is acute myocardial injury in the setting of acute myocardial ischemia. Myocardial infarction is ischemic myocardial injury.
(c) 2021 Pinson & Tang.
Accidental Puncture & Laceration: Coding Clinic 2021 Second Quarter
Does the recent Coding Clinic advice regarding accidental puncture and laceration contradict Official Coding Guidelines for coding Complications of Care? The short answer is No. Here’s why.
In Coding Clinic 2021 Second Quarter, the following scenario was presented: “During a laparoscopic salpingo-oophorectomy, the surgeon noted an incarcerated loop of small bowel adherent to a ventral hernia sac. After take down, the bowel was discolored with multiple serosal tears. The incision was then extended, the loop of bowel was brought out through the incision and the segment with the serosal injury was excised. It seems that serosal tears requiring excision would be clinically significant. However, in this case, the provider documented the injury was inherent to the nature of the procedure. On query, he stated the serosal tear was ‘Unavoidable during extensive lysis of adhesions, not intraoperative complication.’ Would any bowel injury requiring excision be considered clinically significant and reportable? How is the serosal injury and repair by excising the small intestine coded?
In response, Coding Clinic answered, “Assign code K91.71, Accidental puncture and laceration of a digestive system organ or structure during a digestive system procedure, for the serosal injury of the small intestine. Although after query the provider indicated the serosal tear was unavoidable, it was clinically significant, as it required further excision, complicating the surgery.”
Get our CDI Pocket Guide® to learn more about the documentation and coding of complications of care.
This may at first seem contrary to the idea that physician documentation governs code assignment of complications of care; however starting with the 2017 Official Coding Guidelines, Section I.B.16 for Documentation of Complications of Care was modified to read (modification in bold):
“Code assignment is based on the provider’s documentation of the relationship between the condition and the care or procedure, unless otherwise instructed by the classification. The guideline extends to any complications of care, regardless of the chapter the code is located in. It is important to note that not all conditions that occur during or following medical care or surgery are classified as complications. There must be a cause-and-effect relationship between the care provided and the condition, and an indication in the documentation that it is a complication. Query the provider for clarification, if the complication is not clearly documented.”
This phrase “unless otherwise instructed by the classification” was added one year after ICD-10 was implemented in FY2016. This instruction was added to reflect the significant refinement and reorganization of the complication of care codes within ICD-10.
In many situations, complication of care codes are now assigned simply because they occur intraoperatively or postoperatively, and therefore do not require a cause and effect relationship or specific provider documentation that a condition is a “complication.”
In this case, the serosal injury occurring during the procedure is assigned to code K91.71, which specifies “accidental puncture or laceration during a procedure.” Therefore, the Tabular entry governs code assignment.
The serosal injury was clearly documented and was clinically significant particularly since an additional surgical procedure was performed to treat the injury. A query would not be required since the documentation was clear and not conflicting or confusing – even though the surgeon documented it was unavoidable due to extensive lysis of adhesions.
Keep in mind that although conditions classified as complications of care are typically unexpected or unusual outcomes by the care rendered, the term “complication” as used in ICD-10 does not necessarily imply that improper or inadequate care was provided or it was a “surgical misadventure.” And many times it isn’t. Particularly with surgeries, there is always a risk of complications which do occur.
What’s important is for these to be tracked so we have good data to improve the quality and outcomes for our patients. If we’re not coding these conditions when they occur, how can we improve the care we’re providing?
In summary, the ICD-10-CM codes for complications of care, the 2017 Official Coding Guidelines change, and Coding Clinic instruct us to code accidental punctures and lacerations that occur during a surgical procedure that are clinically significant. It is not necessary to query providers for a cause and effect relationship or whether it complicated the procedure. An accidental puncture and laceration code should be assigned unless the documentation is unclear or the condition does not meet the definition of an additional diagnosis.
(c) 2021 Pinson & Tang
Acute on Chronic Respiratory Failure
Case: A 67 year old female with severe COPD and chronic respiratory failure on home oxygen at 2 L/min (28%) is admitted with symptoms of wheezing, cough, chest congestion and increased shortness of breath. She had increased her home oxygen to 4 L/min (36%) with some improvement. Chest x-ray shows COPD without infiltrates; no evidence of pneumonia. Pulse ox reading (SpO2) on 4 L/min is 92%. ABG on oxygen at 4L/min is pH 7.38 / pCO2 55 / pO2 64. What are the diagnoses and why?
Answer: Acute exacerbation of COPD with acute on chronic (hypoxemic) respiratory failure. The diagnosis of acute on chronic respiratory failure can be challenging. An ABG is most helpful in making a diagnosis.
Chronic respiratory failure is caused by abnormalities of oxygenation and carbon dioxide elimination due to chronic lung disease. It may be classified as hypoxemic or hypercapnic.
Chronic hypoxemic: SpO2 < 91% on room air or pO2 < 60 on room air, and/or
Chronic hypercapnic: Elevated pCO2 > 50 (chronic hypercapnea/chronic respiratory acidosis) with normal pH (7.35 - 7.45)
The use of home oxygen is a reliable indicator of chronic hypoxemic respiratory failure since SpO2 ≤ 88% is required to meet medical necessity criteria for home O2.
Acute-on-chronic hypoxemic respiratory failure is an acute exacerbation or decompensation of chronic respiratory failure recognized by worsening dyspnea and the following:
Increase in chronic supplemental oxygen, or
pO2 < 60 or SpO2 < 91% on usual home O2 (rather than room air), or
Decrease in baseline pO2 by > 10 mmHg on ABG
If an ABG were obtained showing acute hypercapnic respiratory failure (pCO2 >50 mmHg and pH <7.35) this diagnosis is easily confirmed. In this case, however, the patient does not have acute hypercapnic respiratory failure because the pH is normal indicating only chronic hypercapnic respiratory failure.
Could she have chronic hypoxemic respiratory failure? Yes indeed, she does because she requires home O2. How about an acute decompensation of chronic hypoxemic respiratory failure? The usual indicators of hypoxemic respiratory failure (pO2, SpO2, pO2/FIO2 ratio) must be interpreted with caution when the patient has pre-existing chronic hypoxemia as this patient certainly does. It is essential to keep in mind that home oxygen is titrated to maintain the patient's pO2 just above 60 mmHg (SpO2 >91%).
In this case, she had increased shortness of breath suggesting an acute fall in oxygenation levels probably below her expected baseline. Worsening symptoms alone suggest an acute exacerbation of her chronic baseline state. The fact that she required a substantial increase in home oxygen from 2 L/min (28%) to 4L/min (36%) to improve symptoms and ultimately went home on her 2 L/minute also indicates an acute decompensation of her baseline state confirming acute-on-chronic hypoxemic respiratory failure.
See further discussion on how to differentiate acute and chronic respiratory failure in the CDI Pocket Guide.
Morbid and Severe Obesity: How are these defined?
Historically, a body mass index (BMI) ≥ 40 has been defined as “morbid” or “extreme” obesity. The World Health Organization (WHO) categorizes obesity by three classes with Class 3 “morbid” or “severe” obesity as BMI ≥ 40.
The “Practical Guide to the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults” was developed by the National Institutes of Health (NIH) and the North American Association for the Study of Obesity using evidence-based methodology for assessing and treating overweight and obese patients.
This report introduced the term “clinically severe” obesity. Clinically severe obesity is defined as: BMI ≥ 40 or a BMI ≥ 35 with serious comorbid conditions that may warrant weight loss surgery.
NIH report, page 4
According to the NIH report, those diseases or conditions that denote serious comorbid conditions and high absolute risk are established coronary heart disease, other atherosclerotic diseases, type 2 diabetes, and sleep apnea. Three or more of the following risk factors also confer high absolute risk: hypertension, cigarette smoking, high low-density lipoprotein cholesterol, low high-density lipoprotein cholesterol, impaired fasting glucose, family history of early cardiovascular disease, and age (male ≥ 45 years, female ≥ 55 years).
The NIH definition conforms to the indications for bariatric surgery. The NIH further indicates that a BMI of 35-39.9 without comorbidity is “obesity.”
From a coding standpoint, ICD-10 code E66.01 includes both “morbid” and “severe” obesity. If morbid or severe obesity is documented for a patient with a BMI 35-39.9 and who has a serious comorbid-related condition, code E66.01 is assigned. On the other hand, if no serious comorbid condition is documented within the record, code E66.01 is not clinically valid.
Get our CDI Pocket Guide® for more information about obesity and BMI.
(c) 2021 Pinson & Tang
Expanding Your CDI Program? Some things to consider...
CDI programs were originally developed to improve the completeness, accuracy, and clarity of inpatient clinical documentation to ensure inclusion of pertinent diagnoses that influence DRG assignment. With the advent of public reporting of quality measures and the CMS pay-for-performance programs, the role of CDI now extends well beyond DRGs. Hospital CDI programs frequently include review of additional payer sources beyond MS-DRGs (APR-DRG, non-DRG), mortality reviews, hospital-acquired conditions (HACs), patient safety indicators (PSIs), and outpatient services.
How can an organization make the most of their CDI services and achieve the greatest return on investment? Given finite resources, CDI will be most effective when you’ve correctly identified the challenges and opportunities that face your hospital. Some of the most fruitful opportunities may be found in:
HCCs in the inpatient setting
Payer denials and appeals
Physician office practice
Emergency department
Observation services
For each opportunity area, you should first identify specific needs and resources (e.g., staffing, collaboration with other departments) and decide how you will measure your results and define success. Wherever possible, baseline data should be generated as a first step to track a return on investment (ROI) for your expanded CDI program activities.
Many hospitals can start with inpatient capture of HCCs, because the additional work effort can usually be absorbed by your current CDI staff. Reducing payer denial risks does not necessarily require additional resources, unless CDI is involved in composing appeal letters.
To expand the scope of CDI to the outpatient setting typically requires more staff. Since payment for an outpatient encounter is determined primarily by the service provided and not the diagnosis coded, however, it can be difficult to demonstrate an objective return on investment to support the effort.
Every hospital is unique. The decision to expand your CDI program into other areas should be made only after consideration of the particular circumstances of your own facility.
INPATIENT HCCs. Capture of HCC diagnoses in the inpatient setting is important since HCCs affect risk-adjustment for payment incentives such as the CMS Pay for Performance programs. Only those HCCs submitted from inpatient discharges are used for risk adjustment of the three CMS inpatient pay for performance programs.
As value-based risk adjustment payment models become more prevalent, accurate documentation of HCC diagnosis codes will become more central to reimbursement.
To incorporate HCCs into your inpatient CDI review process, first optimize the MS-DRG assignment with identification of MCC/CCs and APR-DRG severity levels. Most diagnoses that influence APR-DRG severity are also CCs or MCCs; there are only a few non-CC conditions that can change the APR-DRG severity level.
On the other hand, HCCs tend to be chronic conditions and only half of the CMS-HCCs are CCs or MCCs. For example, a metastatic cancer diagnosis (which is a CC) is the highest-weighted HCC and significantly affects risk adjustment for most outcome measures. This should be a CDI focus to ensure this diagnosis (when supported) is always coded on the claim.
The CDI team should make a list of the more common, high-impact HCC diagnoses to ensure capture and query for these diagnoses as well. Our OutpatientCDI Pocket Guide: Focusing on HCCs includes a list of the most common HCC diagnoses to help you identify your focus list.
It is most effective when processes for capturing chronic conditions that influence risk adjustment within your electronic health record are incorporated systematically by your physician documentation procedures. Links between problem lists and provider notes, a problem list reconciliation process, and physician admission order templates can support point-of-care documentation of these pertinent conditions.
In collaboration with the quality department, the CDI team should review quality and pay-for-performance reports to identify opportunities where more precise physician documentation and coding could improve data quality, risk adjustment, and the hospital’s overall performance results.
Documentation of HCCs is particularly important if your organization or providers are paid under a capitation or value-based contract (e.g., ACO, APM). The impact will vary based on your patient populations and insurance types. In addition to knowing whether your state uses a risk adjustment methodology or value-based contract, you should determine whether your organization or its employed physicians:
Participate in any full-risk capitation agreements
Are part of an accountable care organization (ACO) bundled payment model, or other alternative payment model
Participate in any value-based agreements with Medicare Advantage or other health plans, creating a revenue incentive if quality or risk scores improve
Offers a provider-sponsored Medicare Advantage plan
At this time, most hospitals and providers are not paid under any capitation or value-based contracts, but these are becoming more common.
In our next article, we will discuss CDI and coding involvement in payer denials and appeals.
Filtering Out Confusion Over Kidney Disease
As part of our free webinar series, we conducted a webinar in December 2020 clarifying the diagnostic criteria for acute kidney injury (AKI), acute tubular necrosis (ATN), and acute on chronic kidney disease (CKD). We present the highlights below, including case studies and coding tips.
Over the past twenty years there have been several attempts to come up with diagnostic standards for AKI/renal failure, most notably in JAMA (2003), at the 2004 RIFLE conference, and in the Acute Kidney Injury Network (AKIN) report (2007). Finally, in 2012 the Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Guidelines combined the best of these previous efforts, providing an authoritative diagnostic standard for AKI that is now accepted world-wide.
Get our CDI Pocket Guide® for help with applying the diagnostic criteria for Acute Kidney Injury.
Acute Kidney Injury (AKI)
Seemingly small changes in creatinine reflect a significant loss of renal function: a creatinine increase of 1.5 times the baseline level corresponds to a 25% loss of renal function, and an increase to twice the baseline level corresponds to a 50% loss of renal function. Identifying and treating acute kidney injury as early as possible is therefore crucial.
KDIGO specifies three different criteria for AKI, any one of which is sufficient for diagnosis:
Increase in creatinine to ≥ 1.5 times baseline (within a 7-day period), or
Increase in creatinine of ≥ 0.3 mg/dL within 48 hours, or
Urine output < 0.5 ml/kg/hr for 6 hours
Criterion 1 can be applied either retrospectively orprospectively. The latter is more common, since the baseline creatinine is usually not known upon admission, and the creatinine falls after administration of IV fluids; in such cases, if the creatinine measured at admission is 1.5 times greater than a subsequent measurement within 7 days, this is sufficient for diagnosis. The calculation is simple: divide the highest creatinine level by the lowest.
Clinical case A. A patient is admitted with a creatinine of 2.2 and unknown baseline. Over the next three days, their creatinine falls to 1.3, which is now assumed to be the baseline. To calculate the degree of change, the admission creatinine of 2.2 is divided by the baseline of 1.3, yielding 1.7. Since 1.7 is more than 1.5, the diagnosis of AKI present on admission is confirmed.
Criterion 2 requires no baseline creatinine level and is applied prospectively, as it requires two measurements no more than 48 hours apart to show an increase from the first measurement by at least 0.3 mg/dL. If the second creatinine level is lower than the first, this diagnostic criterion cannot be applied—a point sometimes misunderstood by providers and documentation specialists alike.
Clinical case B. An initial creatinine of 1.3 increases to 1.7 in 36 hours. This 0.4 mg/dL increase from the initial level confirms a diagnosis of AKI.
Clinical case A, revisited. The patient's creatinine fell from 2.2 to 1.8 within 48 hours. This patient did not meet Criterion 2, because the creatinine fell; at 48 hours the patient did not meet Criterion 1, either, because 2.2 divided by 1.8 is less than the required 1.5. In another 24 hours, however, as the creatinine fell further to 1.3, the patient met Criterion 1 for AKI.
Criterion 3 for urinary output is straightforward but less commonly encountered. The urine output calculation is quantity of urine in ml divided by patient's weight in kg divided by 6 hours.
Clinical case C. A 150-pound (68 kg) septic patient has urine output of only 180 ml over 6 hours. 180 ml / 68 kg / 6 hour = 0.44 ml/kg/hour. This meets Criterion 3 for AKI.
Acute Tubular Necrosis (ATN)
ATN is defined as AKI due to impairment of renal tubule function. It is a clinical diagnosis based on the persistence of AKI with creatinine levels above baseline for at least 72 hours. ATN is most commonly caused by IV contrast, prolonged hypotension or shock, medications, chemicals, toxins, prolonged pre-renal AKI, rhabdomyolysis with myoglobinuria, or tumor necrosis syndrome. AKI due to contrast or myoglobinuria is always caused by ATN.
In the majority of cases, there is no actual necrosis, which is a sign of very severe injury. "Acute tubular injury" would therefore be a more accurate term for this condition overall, but this new terminology has not been officially accepted.
Coding tip: It is important to distinguish AKI from ATN, since the code for AKI is a CC while ATN is an MCC.
Urinalysis. Urine chemistries may be used to confirm ATN in questionable cases or rule out other diagnoses. Urinary sodium concentration > 40 meq/L and fractional excretion of sodium (FENa) > 2% help confirm the ATN diagnosis but are not required. If the problem is, instead, pre-renal AKI (e.g., dehydration), the urinary sodium concentration is expected to be < 20 meq/L and FENa < 1%. Note that since the vast majority of cases of ATN are functional (without necrosis), the urine sediment will be unremarkable. (“Muddy brown casts” and renal tubular cells appear in the urine only with severe ATN that has led to necrosis)
Clinical case D. A 58-year-old is admitted with pulmonary embolism, confirmed by CT angiography. Creatinine levels measured over six days were as follows: 0.5, 1.0, 1.4, 1.6, 1.2, 0.8. In this case, the baseline creatinine was 0.5 and increased to 1.0 in one day, which meets the AKI criterion of creatinine increase > 0.3 within 48 hours. Creatinine remained above baseline for 4 days (> 72 hours) and at discharge, meeting the criterion for ATN. (This was an easy one: AKI due to IV contrast is always ATN.)
Acute on Chronic Kidney Disease (CKD)
Acute on chronic kidney disease is simply the occurrence of AKI in the setting of pre-existing CKD, which makes patients extremely vulnerable to any physiological stress. Separate codes are assigned for AKI and CKD by stage, as ICD-10 has no combination code for this situation. AKI criteria for CKD patients are precisely the same as for non-CKD patients (see first section above).
For CKD to be diagnosed, either of the following criteria must be present for > 3 months:
The CKD stage is determined by the stable GFR. The GFR may fluctuate during the inpatient stay, so the "stable GFR" will be the GFR at or near the time of discharge.
Stage
GFR
1
≥90
2
60-89
3a
45-59
3b
30-44
4
15-29
5
<15
ESRD
Dialysis-dependent stage 5
Note that, because the GFR in Stages 1 and 2 is > 60, thereby failing to meet the first criterion, a diagnosis of CKD in those cases will require the finding of at least one clinical marker of kidney injury. Stages 3-5 CKD often have clinical markers of kidney injury, but these are not required because the GFR in these cases is, by definition, < 60.
Coding tip: Correct documentation of CKD stage is important, since stages 4 and 5 are CCs, while stages 1-3 are non-CCs. If the stage is not documented, providers should be queried for patients with a stable GFR < 60.
Clinical case E. A 60-year-old male with CKD-4 was admitted for COVID-19 and pneumonia with a creatinine level of 4.4 and GFR of 14. His creatinine level fell to 2.5 and GFR improved to 27 by the time of discharge. The creatinine at admission (4.4) is 1.8 times the lowest creatinine level (2.5), which meets the AKI criteria of > 1.5 times or more from baseline. The discharge GFR of 27 confirms stage 4 CKD.
Our live interactive webinars provide accessible, cost-effective training for teams or larger groups. Contact us if you’re interested in our webinars or consultative services.
(c) 2021 Pinson & Tang
Important COVID-19 Updates
In another unprecedent mid-year ICD-10 classification update, new COVID-19 related codes have been created effective January 1, 2021. The new COVID-19 related ICD-10-CM codes are:
J12.82
Pneumonia due to coronavirus disease 2019
M31.81
Multisystem inflammatory syndrome
M35.89
Other specified systemic involvement of connective tissue
Z11.52
Encounter for screening for COVID-19
Z20.822
Contact with and (suspected) exposure to COVID-19
Z86.16
Personal history of COVID-19
There are also 21 new procedure codes to describe the introduction or infusion of therapeutics, including monoclonal antibodies and vaccines for COVID-19 treatment—although these codes will not affect DRG assignment. Medicare will pay for the COVID-19 vaccines and their administration separately from the DRG rate. The CPT codes should be reported when the vaccine is administered while a hospital inpatient.
Medicare Requirement for 20% Add-On Payment Requires Positive Test Result. Effective with admissions occurring on or after September 1, 2020, claims eligible for the 20 percent increase in the MS-DRG weighting factor will also be required to have a positive COVID-19 laboratory test documented in the patient’s medical record. The viral test can either be performed during the hospital admission or within 14 days prior to the hospital admission.
Although the Official Coding Guidelines state that the provider’s documentation that the individual has COVID-19 is sufficient to code U07.1, claims eligible for the additional 20% now require a positive test result in the medical record which wasn’t required prior to September 1.
CMS may conduct post-payment audits to confirm the presence of a positive COVID-19 laboratory test and recoup the 20 percent increase if no such test is contained in the medical record. Although hospitals should continue to code U07.1 when the diagnosis meets the official coding guidelines definition of COVID-19, if the record does not have evidence of a positive test result hospitals can decline the additional payment at the time of claim submission to avoid the repayment.
The Solution to Severe Malnutrition Denials: Document the Treatment!
The CMS Office of Inspector General (OIG) released a report in July 2020 claiming that hospitals over-billed Medicare approximately $1 billion in a two-year period for claims that included a secondary diagnosis of severe malnutrition.
The OIG audited 200 claims randomly selected from a total of 224,175 claims from fiscal years 2016 and 2017 that contained code E43 (unspecified severe protein-calorie malnutrition) or E41 (nutritional marasmus) which are classified as MCCs.
Severe Malnutrition OIG Audit Findings
OIG audit findings. The auditors found that, in 164 of the 200 claims reviewed, the diagnosis of severe malnutrition was not clinically supported. The denials were based on ASPEN diagnostic criteria and lack of evidence that the treatment was congruent with the severity of illness in intensity and complexity. In other words, many of the 164 claims failed to show the complex decision-making and intense intervention expected for severe malnutrition.
Clinical validation of severe malnutrition. For many years, ourCDI Pocket Guide® has cautioned hospitals and providers that the clinical validity of any diagnosis depends, in part, on providing the management expected for the condition. For example, a diagnosis of gram-negative or staph pneumonia will not be considered clinically valid if azithromycin is the only antibiotic administered; a diagnosis of acute kidney injury (AKI) will not be considered clinically valid without hydration and monitoring of creatinine levels for improvement.
In the case of severe malnutrition, things become a bit more complicated since many patients may meet two ASPEN criteria for severe malnutrition but not receive the intense management or treatment expected with this diagnosis. Much like marasmus and kwashiorkor in underdeveloped countries, severe protein-calorie malnutrition (code E43) in the United States should be considered a serious, potentially life-threatening situation requiring carefully monitored, aggressive management.
What treatment is congruent with severe malnutrition? While a patient who has non-severe malnutrition may be seen by a nutritionist, who would likely recommend a nutritious diet along with one to two daily liquid supplements (e.g., Boost), a patient with severe malnutrition would be expected to receive some of the following:
Two to three daily liquid supplements
Daily calorie counts, frequent weighing
Appetite stimulants (Megestrol)
Frequent follow-up with a nutritionist or other healthcare provider
Lab monitoring (e.g., electrolytes, including phosphate and potassium)
Parenteral or enteral nutrition: While TPN (total parenteral nutrition) is typically used only for severe malnutrition, enteral nutrition (G-tube or NG feeding tube) may be used for other conditions such as severe dysphagia / frequent aspiration, severe debilitating dementia, esophageal motility disorders, esophageal obstruction.
Let's look at two cases to illustrate the difference.
Case study #1: A 91-year-old female with a history of dementia was admitted with rectal pain and severe fecal impaction. Colonoscopy revealed stercoral colitis and multiple mucosal ulcers. The gastroenterologist diagnosed “severe protein-calorie malnutrition.” The nutritionist documented “inadequate calorie intake; 8% weight loss in last 1.5 months” and “high risk.” The patient’s BMI was 24 (upper end of normal). The patient was treated with IV Cipro and Flagyl, advancement of diet as tolerated, with Boost twice a day.
Case study #2:An 80-year-old female with congestive heart failure who lives alone at home was admitted after two weeks of increasingly severe diarrhea and abdominal pain. She had been recently treated with antibiotics for recurrent urinary tract infection. Physical exam revealed a frail, thin female who needs assistance getting up from a chair and generalized weakness. Lab results included CRP 5.5 (range 0.3-1.0), albumin 2.8 (range 3.4-5.4); prealbumin 11.0 (range 15-36), and positive C. diff toxin. She was diagnosed with C. diff colitis and transferred to rehab after a five-day hospital stay. The nutritionist documented a 6% weight loss over the past month and a BMI of 19.3. Appetite was poor and the patient consumed < 75% calories for 3 weeks. No obvious muscle mass or subcutaneous fat loss. She was treated with Boost 3-4 times daily and daily calorie counts to monitor calorie intake.
Which of these patients would be considered to demonstrate "severe” malnutrition?
Patient #1 meets the ASPEN criteria for severe malnutrition due to reduced calorie intake and weight loss in an acute setting, but her treatment (Boost twice a day) would likely be interpreted as mild or moderate malnutrition, despite the fact that her dementia likely means she will need ongoing nutritional monitoring. Also, her BMI indicates she is not severely malnourished. Patient #2 meets GLIM (but not ASPEN) criteria for severe malnutrition, because of her BMI of 19.3 (< 22 if ≥ 70 years old), documented reduced nutritional intake for over two weeks, and evidence of acute disease with severe systemic inflammation (C. diff colitis with elevated CRP). The patient’s documented treatment (3-4 daily liquid supplements plus daily calorie counts) is more consistent with a diagnosis of severe malnutrition.
How to prevent malnutrition denials. As usual, the answer is in the documentation—of both the diagnostic criteria met and the treatment that matches the severity of the diagnosis.
Select either the ASPEN or GLIM criteria, not both. Hospitals should establish a diagnostic standard and organization guidelines for malnutrition and involve the compliance department. Choose either ASPEN or the more recent international GLIM criteria and use the criteria consistently across the institution. Be sure your nutritionist documentation includes the specific ASPEN or GLIM criteria that are met. Educate clinicians.
Ensure the treatment plan is as intense as the diagnosis is severe. If the treatment plan does not contain some of the treatment indicators above for "severe malnutrition," the diagnosis of severe malnutrition is likely to be considered invalid.
Appealing severe malnutrition denials. As a result of this audit, CMS has instructed its audit contractors to recover the 164 identified overpayments and to review additional claims from the 224,000+ audit sample to recover additional overpayments for severe malnutrition. So, get ready to defend your claims.
Do not appeal all denials. If after a review of the medical record, the documentation clearly does not meet the clinical criteria or treatment expected for severe malnutrition, do not appeal—it will waste everyone’s time.
If the diagnosis of severe malnutrition is clinically supported, however, include these three elements in your appeal letter:
High-risk patient: Any past medical history, social/environmental issues, or current conditions that support a high risk for malnutrition.
Diagnostic criteria: The specific diagnostic criteria that are supported by the medical record findings – either ASPEN or GLIM.
Treatment: The intensity of treatment that fits the diagnosis.
In the above case studies, case #1 would likely not succeed in an appeal.
Although the OIG audit suggests that severe malnutrition is over-reported, the major nutrition societies report widespread under-recognition and under-treatment of malnutrition. Clearly, there is a need for authoritative diagnostic standards and clinician education, but the best way we can help determine the prevalence of malnutrition is to ensure accurate medical record documentation.