Most pulmonary emboli (PE) arise from deep venous thrombosis (DVT) of the proximal veins of the lower extremities (iliac, femoral, and popliteal). The clinical presentation of pulmonary embolism is variable and often nonspecific, making the diagnosis challenging. DVTs are dangerous since they can result in PE which can be deadly.
The underlying causes of DVT and PE may be hereditary (genetic mutations) or acquired. Hereditary causes are rare and include Factor V Leiden, elevated Factor VIII, and deficiencies in protein S, protein C, and antithrombin.
Acquired causes are more common. Precipitating factors for DVT and subsequent PE, include:
Immobilization due to hospitalization, travel, obesity, or stroke;
Adverse effects of drugs, such as steroids, oral contraceptives, anticoagulants, and heparin;
Clinical conditions including major trauma, pregnancy, malignancy, diabetes, and myeloproliferative disorders; and
Autoimmune diseases such as lupus anticoagulant and antiphospholipid syndrome.
Immobilization leads to venous stasis with accumulation of clotting factors and fibrin, resulting in blood clot formation.
Healthcare-associated venous thromboembolism (VTE) is a result of hospitalization, surgery, or other healthcare treatment or procedure. According to the CDC, although anyone can develop a DVT, over half are related to a recent hospitalization or surgery and most occur after discharge; approximately 70% of these could be prevented.
Acute, Chronic, or "History of" DVT and PE
The acuity of DVT and PE should be identified for clinical and coding purposes:
Acute,
Chronic, or
“History of”
AcuteDVT or PE is usually treated with heparin-type medications for immediate anticoagulation to prevent further clot growth. None of these medications actually “treat” the acute DVT. The acute blood clots are usually dissolved spontaneously by endogenous processes in the veins within a few days, not by heparin, Coumadin, or Xarelto. A transition is then made to intermediate term (3-12 months) Xarelto or Eliquis, to prevent recurrent DVT/PE.
The first episode of PE or DVT is acute until the clot(s) have resolved – approximately 10-14 days. After that it should be considered resolved, i.e., “history of”, even though anticoagulation to prevent a recurrence is continued up to one year. A subsequent DVT/PE episode requiring admission (or not) would constitute a "recurrent" episode of acute DVT or PE.
Chronic DVT is a residual clot or fibrosis of a clot that continues to cause deep venous obstruction resulting in edema, pain, or chronic venous ulcers. Chronic PE is a persistent clot or fibrosis causing blockage in pulmonary arteries and chronic pulmonary hypertension. Both require life-long (> 1 year) anticoagulant therapy, such as Eliquis, Xarelto, or Coumadin.
The acute episode of DVT and PE ends when the patient is stabilized, transitioned to Eliquis or Xarelto, and discharged. If such a patient is admitted with “history of DVT (or PE)” and without residual clot or symptoms, the correct status is “history of” DVT/PE, not acute or chronic DVT/PE.
CDI, or Clinical Documentation Integrity, can be understood as a process aimed at improving the accuracy of medical record documentation and coding for quality and reimbursement purposes. Throughout this article we will discuss the evolution of clinical documentation and the strategies and guidelines used today as explained in the CDI Pocket Guide®.
A Brief History of Clinical Documentation
Before answering the question “what is CDI” we have to give a brief history. Prior to 1983, hospitals would bill Medicare or the insurance company based on a charge for every supply and service provided, such as medications, bandages, labs, x-rays, daily room and bed charge, and Medicare would pay a percentage of these “total charges.” This caused long hospital stays where as many services as possible were done for the patient, i.e., the more services provided, the higher the reimbursement.
Inpatient Prospective Payment System (IPPS)
As a result, the Inpatient Prospective Payment System (IPPS) was introduced by the federal government in 1983 to curb skyrocketing healthcare costs for Medicare patients. The objective of the IPPS was to change hospital behavior through financial incentives that encourage more cost-efficient management of medical care. Under the IPPS, hospitals are paid a predetermined, fixed rate based on average costs for each medically necessary Medicare inpatient admission based on a diagnosis-related group (DRG).
Diagnosis-Related Group
The DRG system is an inpatient classification scheme that categorizes patients who share similar clinical characteristics and costs. Each inpatient discharge is classified into a DRG based on the numerical ICD-10 coded data submitted by the hospital on the billing claim.
Selecting the Appropriate ICD-10 Code
ICD-10 coding is the process of transforming disease, injury, and procedure descriptions into alpha-numeric codes. ICD-10-CM (International Classification of Diseases, Tenth Revision, Clinical Modification) is the coding classification system used to code diagnostic and operative procedural data for official morbidity and mortality statistics in the United States.
The ICD-10 billed codes must be supported by the medical record documentation of the physician and substantiated by clinical findings. For example, if the hospital bills a diagnosis code for pneumonia, physician documentation must include a diagnosis of pneumonia, and the clinical findings and treatment provided must also substantiate it. This is why correct CDI is so important.
Ensuring the Correct Principal Diagnosis
Correctly identifying the principal diagnosis and significant surgical procedures are the most important factor in DRG assignment. The principal diagnosis code is the first code listed on the hospital claim and is defined as “that condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care.” The coding professional must assign the principal diagnosis based on all physician documentation found in the entire record applying official coding guidelines and instructions which are usually unfamiliar to physicians.
All other conditions either present on admission or that develop subsequently may qualify as secondary diagnoses if they affect patient care. CMS has designated certain of these conditions as CCs (comorbidities or complications) and MCCs (major CCs) that may affect DRG assignment.
Determining the DRG Payment
The DRG payment for a hospital inpatient is determined by multiplying the relative weight for the DRG by the hospital’s payment rate. Medicare calculates the DRG relative weights and hospital blended payment rates annually.
For example, a patient admitted with a principal diagnosis of congestive heart failure is assigned to DRG 293 (Heart Failure w/o CC/MCC), which has a relative weight of 0.5899. If the hospital payment rate is $7,000, the hospital’s reimbursement for this patient is determined by multiplying 0.5899 by $7,000. The payment to the hospital for this patient would be a flat fee of $4,129.
The DRG relative weight reflects the expected average length of stay, severity of illness, resource utilization and the relative cost of treating patients in this DRG.
The coding process is extremely important since it determines what DRG will be assigned for a patient, which, in turn, determines hospital reimbursement. Coding an incorrect principal diagnosis or procedure or failing to code a pertinent secondary diagnosis can significantly affect DRG assignment and the hospital reimbursement. Coded data is also used to determine physician reimbursement, publicly reported physician and hospital profiles, mortality and complication ratings, and other outcome measures.
The Benefits of Clinical Documentation Integrity
So, to fully understand “what is CDI”, let’s talk about the program itself. A Clinical Documentation Integrity (CDI) program is designed to clarify imprecise and incomplete provider documentation. A CDI program not only helps physicians with documentation improvement but ensures the correct translation of physician documentation to the proper ICD-10 codes submitted on the hospital claim. This in turn will ensure that the illness severity in patients is accurately reflected, and proper payment for the care provided is received.
The CDI team is multidisciplinary and includes clinicians, clinical documentation specialists, and coders. All these stakeholders play a crucial role in ensuring precise documentation and correct coding that accurately reflects the true illness severity of our patients.
Clinical Documentation Integrity Specialists
Clinical Documentation Integrity (CDI) Specialists are employed by hospitals to concurrently review patients’ medical records, assign a working DRG and determine if the documentation accurately reflects severity of illness if the patient. The CDI specialist queries clinicians for clarification when an improvement opportunity is identified, such as clinical findings supporting a more specific or additional diagnosis not yet documented, or when there is conflicting or confusing diagnostic or procedural information. Clear and precise documentation paints the true nature of the patient’s condition that supports correct coding and DRG assignment.
Why is this important? In addition to hospital reimbursement, physician documentation drives practically all the major quality outcome measures. Outcome measures are used to stratify the performance of hospitals and physicians from best to worst. Medicare, Healthgrades, and news organizations such as US News and World Report publicly report hospital and physician quality and outcome measures.
How CDI Works
Hospital reimbursement and outcome measures are derived from the documentation in the medical record which are translated by the coder into ICD-10 codes on claim forms. Billing claims with the ICD-10 codes are submitted to Medicare, Medicaid and commercial payers. All claims data is stored in databases and analyzed to evaluate many aspects of healthcare. The largest is Medicare’s claims database, called MedPAR, which is used by many agencies and organizations to generate outcome and performance measures, such as mortality rates, complication rates, readmission rates, and costs.
For example, CMS HospitalCompare.com publishes hospitals' reported mortality rates for COPD, heart attack, heart failure, pneumonia, stroke, and coronary bypass surgery based on a star-rating. One star is defined as “worse than expected”, three stars is “as expected” and five stars is for “better than expected”. This information is publicly available and may discourage patients from seeking care at this hospital. But is the quality of care poor, or is there actually a documentation or coding problem that is creating a false picture of performance?
An 80-year-old female with preexisting cachexia and 30-pound weight loss in the past three months is admitted with UTI, blood pressure 70/50, heart rate 130, respiratory rate 28, pulse oximetry 85% on room air, WBC 25,000, lactate 4.2. Her hospital length of stay was 6 days, and she expired.
Sepsis due to UTI Septic shock Respiratory failure Severe malnutrition
The above illustrates how physician documentation may influence the reporting of sepsis mortality rates. Provider A’s documentation included urosepsis which is classified as a simple UTI, and hypotension, hypoxemia, leukocytosis, and cachexia are classified as rather insignificant findings in the absence of specific diagnoses. Severity of illness for this case is classified as nothing more than a UTI with no significant comorbidity. Had physician documentation been more precise and specific as shown for Provider B, the illness severity and high risk of mortality would have been more accurately reported, that is, septic shock with respiratory failure and severe malnutrition.
What Is CDI - A Summary
In summary, when you ask, “what is CDI”, this refers to the documentation that drives nearly all the major outcome measures and reimbursement. Precise physician documentation that translates into the correct codes to accurately reflect the patient’s severity of illness is absolutely necessary.
CDI experts, Dr. Richard Pinson and Dr. Cynthia Tang, understand the importance of accurate documentation and have developed an all-encompassing CDI Pocket Guide® to help hospitals and providers improve the efficiency and accuracy of medical record documentation and coding.
Click now to learn more about CDI resources and programs.
Acute MI due to Coronary Artery Stent Stenosis: Coding Challenges
In our recent Cause and Effect webinar we described the ICD-10 E/M convention for which, in certain conditions, the etiology (cause) must be assigned as the principal diagnosis followed by the manifestation (effect). For example, with malignant pleural effusion, code first the neoplasm.
For patients admitted with acute myocardial infarction due to stent stenosis, the E/M convention applies. The ICD-10 classification instructs us to “code first (if applicable)” I97.190, Other postprocedural cardiac functional disturbance following cardiac surgery, when associated with I21.A9, Other myocardial infarction, and T82.855A, Stenosis of coronary artery stent.
We were asked whether code I97.190 should be assigned only when it occurs intraoperatively or following a recent coronary artery stent insertion.
Code I97.190 as principal diagnosis is supported by:
As noted above, the ICD-10 coding convention “etiology/manifestation” instructs us to “code first, if applicable” I97.190 when assigning code I21.A9 for an acute MI.
Code I21.A9 includes Type 3, 4, and 5 myocardial infarctions and any MI associated with revascularization procedure. Type 4 myocardial infarctions are "related to" PCI, stent thrombosis, and restenosis of the stent, and Type 5 is related to CABG. Therefore, I97.190 would be “applicable” to any of these except a Type 3 myocardial infarction, which is defined as “MI resulting in death when biomarker values are unavailable.”
Code I97.190, Other postprocedural cardiac functional disturbance following cardiac surgery, includes both “postprocedural” and “following cardiac surgery.” There is no defined time frame for “postprocedural” or “following cardiac surgery”. The classification does not define a time limit for the development of a complication. It may occur during the hospital episode in which the surgery was performed, shortly thereafter, or years later (Coding Clinic 2002 Second Quarter p. 12-13).
In Coding Clinic 2019 Second Quarter p. 32, in response to a question regarding the “correct diagnosis codes and sequencing of an acute myocardial infarction (MI) due to stent thrombus following coronary angioplasty and stent placement,” Coding Clinic advised to assign code I97.190 as principal diagnosis followed by codes T82.855A and I21A9.
Although assigning both the I97 and the T-code appears redundant since both are complication codes, and the T code specifically describes the stent complication, the ICD-10 classification requires the I97 code to be assigned as principal diagnosis.
Apparently conflicting with the 2019 Coding Clinic advice and the ICD-10 classification are two 2021 Coding Clinics regarding the same circumstances which do not include the I97.190 code. One of the 2021 Coding Clinics addressed a physician diagnosis of the “culprit lesion” essentially saying it identifies the lesion causing an MI. The other involves an MI due to both stent stenosis and progression of native CAD. The omission of I97.190 appears to have been an oversight by the 2021 Coding Clinics since the ICD-10 classification takes precedence. This discrepancy should be explained by Coding Clinic.
It is important to distinguish in-stent stenosis/restenosis, thrombosis, or total occlusion of a stent from progression of coronary artery disease (CAD) which occurs in a native vessel or graft and does not apply to stents.
Bottom line, from a DRG assignment standpoint, whether the I97 code or the specific T82 code is assigned as principal diagnosis, the resulting DRG assignment is DRG 246 with the MI as an MCC. Either the I97 code is assigned (code first) or T code since any treatment or procedure will be directed to the T code stent complication (stenosis, thrombosis), not the myocardial infarction.
Get our CDI Pocket Guide® for more help with "Cause and Effect" and principal diagnosis coding guidelines.
Coagulation Disorders: Hereditary and Acquired Hypocoagulopathies (Hemorrhagic Disorders)
Coagulation disorders are disorders of the bloodclotting factors that disrupt the body's ability to control blood clotting, resulting in either abnormal bleeding or excessive blood clotting. Either can be hereditary or acquired. The general terms “hypo-coagulopathy” is defined as an increased tendency toward bleeding and “hyper-coagulopathy” as an increased tendency toward blood clotting (thrombosis), respectively.
In this article, we will focus on the hypocoagulopathies, i.e., coagulation disorders causing hemorrhage.
There are 12 blood clotting factors, Factors I-V and VII-XIII. All the blood clotting factors are produced by the liver, except Factor IV. Vitamin K is needed for the liver to produce Factors II, VII, IX, X. Phospholipids are components of the cellular and platelet membranes and provide a surface for the chemical reactions of coagulation to take place.
What can disrupt the coagulation process? Many things can, including:
Low, elevated, or defective (genetic mutations) clotting factors
Severe liver disease – Since all, except one, of the clotting factors are produced by the liver, severe liver disease can disrupt the clotting factors. A deficiency of Vitamin K which is needed by the liver can also cause deficiency (needed by the liver)
Antibodies from autoimmune disease
Inhibitors to coagulation factors, also known as circulating anticoagulants, are antibodies that neutralize specific clotting proteins, thereby interfering with their normal function. Antibodies may be directed against isolated clotting factors, as is the case with factor VIII or IX inhibitors.
Drug induced – This is the most common (along with liver disease)
Hereditary hypocoagulopathy, or hemophilias, are very rare and include Von Willebrand disease (VW factor deficiency or abnormality), Hemophilia A (clotting Factor VIII deficiency) and Hemophilia B (clotting Factor IX deficiency.
Acquired hypocoagulopathies are common and usually due to drugs that interfere with normal clotting factors, such as anticoagulants like Coumadin and Eliquis, or antithrombotic drugs that interfere with platelet function like aspirin or Plavix. Severe liver disease causes decreased production of clotting factors, and autoimmune diseases may be associated with inhibitors of clotting factors, e.g., lupus anticoagulant or antiphospholipid antibodies.
Get our CDI Pocket Guide® for more help with identifying coagulation disorders.
How are these acquired hypocoagulopathies identified?
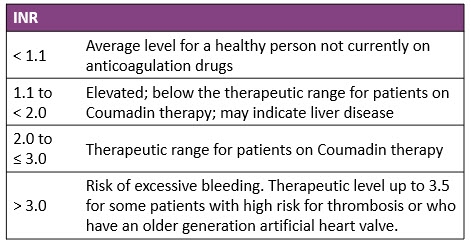
Prothrombin time (PT). Prothrombin is a crucial clotting factor made by the liver. The prothrombin time (PT) is a test that measures how long it takes for a clot to form in a blood sample. The international normalized ratio (INR() is a standardized calculation based on the PT. The PT/INR determines if the blood is clotting normally and measures the therapeutic effectiveness of Coumadin for patients with atrial fibrillation, thromboembolism, stroke, etc. An elevated INR may represent a therapeutic effect or adverse reaction when it causes bleeding.
Below are the INR values and what these indicate:
Other reasons for a high INR include inherited or acquired clotting factor deficiency (I, II, V, VII, X), DIC, Vitamin K deficiency and liver disease.
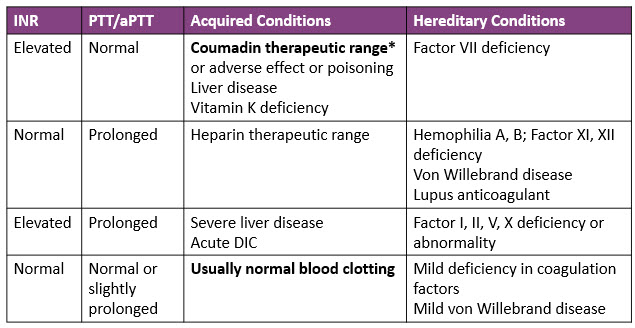
Partial thromboplastin time (PTT). The partial thromboplastin time (PTT) is the time in seconds it takes plasma to clot and measures a different set of clotting factors than the PT. The normal range is 60-70 seconds. Activated PTT (aPTT) is the same test as PTT, but an activator is added that speeds up the clotting time and test results. The normal range is 30-40 seconds. PTT/aPTT are also used to measure the effectiveness of heparin therapy. Patients on Heparin should have a PTT or aPTT 2 to 2.5 times the normal range.
These laboratory findings may indicate:
*
*For patients on Coumadin therapy: Expected therapeutic range for INR is 2.0 to 3.0. For some patients who have a high risk for thrombosis, the INR needs to be higher: 2.5 to 3.5.
For patients who are presurgical: Coumadin is held and INR/PTT should be ≤ 1.5 (there are some exceptions where it must be normal) to reduce the risk of bleeding. Patients not on Coumadin: INR should be normal (<1.1) or cause investigated.
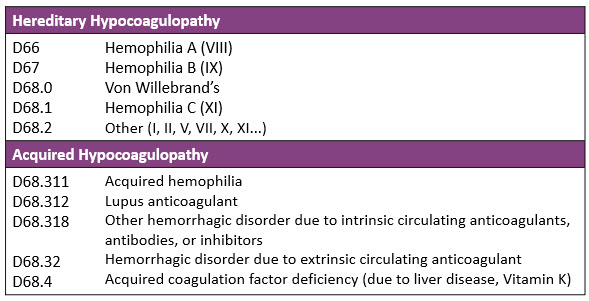
ICD-10 codes for hereditary and acquired hypocoagulopathies are:
Other ICD-10 codes that are not coagulation disorders include:
R79.1, Abnormal coagulation profile: This code should be assigned for patients on anticoagulant therapy, and the PT/INR is elevated, but not causing bleeding.
Z79.01 Long term use (current) of anticoagulants: This code should be assigned for patients on anticoagulant therapy, and the PT/INR is in therapeutic range.
Principal Diagnosis Sequencing: When an anticoagulant or antithrombotic causes the adverse reaction of bleeding, sequencing of D68.32, Hemorrhagic disorder due to extrinsic circulating anticoagulants, and the cause/site of bleeding depends on the circumstances of admission. Was the “focus” of the admission the bleeding itself (e.g., evaluation, procedures, transfusion, monitoring, H/H) or the correction of the bleeding disorder (e.g., vitamin K, fresh frozen plasm)?
Example cases: Test your skills!
Case 1. Patient with epistaxis and taking Coumadin as prescribed; nosebleed treated with nasal packing. Admitted with INR 6.8, treated with fresh frozen plasma to reverse elevated INR, discontinuation of Coumadin, serial hemoglobin and INR, and subsequent cautious resumption of Coumadin based on INR.
Here the principal diagnosis is D68.32, Hemorrhagic disorder due to extrinsic circulating anticoagulants [if documented]. Secondary diagnoses include T45.515A, Adverse effect of anticoagulants, and R04.0, Epistaxis. The hemorrhagic disorder was the focus of the admission and an adverse effect of Coumadin.
If Coumadin was taken improperly, i.e., poisoning, the poisoning code (T45.511- or T45.521) would be sequenced first.
Case 2. Patient admitted with GI bleeding while properly taking Plavix. Treatment included discontinuation of Plavix, blood transfusion, EGD and colonoscopy, which was identified a bleeding gastric ulcer.
The principal diagnosis in this case is K25.4, Gastric ulcer with bleeding. Secondary diagnoses include D68.32, Hemorrhagic disorder due to extrinsic circulating anticoagulants [if documented], and T45.525A, adverse effect of antithrombotic. The ulcer with bleeding was the focus of the admission and an adverse effect of Plavix (antithrombotic).
Cases 3 to 5: Surgical patient
Case 3. 52-year-old female, morbidly obese, admitted for exploratory lap, abdominal hysterectomy/BSO for uterine fibroids on Oct. 26. Patient was noted to have considerable post-operative incisional bleeding due to subcutaneous hematoma, return to OR for wound exploration and closure.
Pt on Coumadin held for surgery and Lovenox given. Labs 10/26: PT 18.3/INR 1.61.
This clinically indicates: D68.32, Hemorrhagic disorder due to extrinsic circulating anticoagulants.
Case 4. 52-year-old female, morbidly obese, admitted for exploratory lap, abdominal hysterectomy/BSO for uterine fibroids on Oct. 26 without complication.
Pt on Coumadin held for surgery and Lovenox given. Labs 10/26: PT 18.3/INR 1.61. PN: Elevated PT/INR.
An abnormal PT/INR or PTT due to an anticoagulant that does not cause bleeding is assigned code R79.1, Abnormal coagulation profile.
Case 5. 52-year-old female, morbidly obese, admitted for exploratory lap, abdominal hysterectomy/ BSO for uterine fibroids on 10/26 without complication.
Pt on Coumadin held for surgery and Lovenox given; INR 1.1.
The PT/INR is in the therapeutic range. Assign code Z79.01, Long term (current) use of anticoagulants.
Coagulation Disorders: Primary and Secondary Hypercoagulable States
Coagulation disorders are disorders of the blood clotting factors that disrupt the body's ability to control blood clotting, resulting in either abnormal bleeding or excessive blood clotting. Either can be hereditary or acquired. The general terms “hypo-coagulopathy” and “hyper-coagulopathy” are defined as an increased tendency toward bleeding and an increased tendency toward blood clotting (thrombosis), respectively.
Primary (Hereditary) Hypercoagulable State, or Primary Thrombophilia, is caused by several rare genetic abnormalities. Factor V Leiden is the most common; others include elevated Factor VIII, and deficiencies in protein S, protein C and antithrombin. As with acquired thrombophilia, it is not typically identified until a thrombosis occurs, but can be diagnosed with various blood tests, such as lupus anticoagulant (LA) panels, activated protein C resistance, protein C and protein S activity, antithrombin activity, and genetic tests.
Secondary (Acquired) Hypercoagulable State, or Acquired Thrombophilia, are due to underlying systemic diseases or clinical conditions and cannot be identified until a thrombosis occurs.
Acquired thrombophilia has many causes or precipitating factors such as:
Immobilization (due to hospitalization, travel, obesity, stroke, etc.): Local venous stasis by accumulation of clotting factors and fibrin resulting in blood clot formation.
Adverse effect of drugs: steroids, oral contraceptives, anticoagulants, heparin
Clinical conditions: Major trauma, pregnancy, malignancy, diabetes, myeloproliferative disorders
Autoimmune disease: Lupus anticoagulant and antiphospholipid syndrome (APS)
Patients who are “high risk” for thrombosis cannot be diagnosed with a hypercoagulable state until a thrombosis occurs. Likewise, if a thrombosis occurs due to immobilization, adverse effect of drugs, trauma, pregnancy, etc. and the precipitating factor is no longer present, the patient is no longer in a hypercoagulable state.
Treatment of thrombosis and acquired thrombophilias such as lupus anticoagulant and APS involves anticoagulants like warfarin, heparin, direct factor Xa inhibitors (rivaroxaban, apixabn, and edoxaban), and and direct thrombin inhibitors (dabigatran).
ICD-10 Coding of Hereditary and Acquired Thrombophilia
A 2021 Coding Clinic advised to assign code D68.69, Other thrombophilia, for a provider diagnosis of “secondary hypercoagulable state.” The case described a 79-year-old with a history of paroxysmal atrial fibrillation on anticoagulant maintenance who is diagnosed with secondaryhypercoagulablestate.
A hypercoagulable state in a patient on chronic anticoagulant therapy for atrial fibrillation would be extremely rare, since this is the direct opposite reaction of anticoagulant therapy, which is to prevent hyper-coagulopathy (thrombosis). Hypo-coagulopathy is the therapeutic effect of anticoagulant therapy, and abnormal bleeding is a common adverse effect (code D68.32).
Do not query for secondary hypercoagulable state in patients on anticoagulant therapy, unless paradoxical thrombosis occurs, and the anticoagulant therapy is discontinued.
The diagnosis of acquired thrombophilia depends on the clinical presentation described above.
COVID-19 and Hypercoagulable State
Recent clinical studies have found a high incidence of pulmonary embolism (PE) and deep vein thrombosis (DVT) in COVID-19 patients.
The development of hypercoagulability (PE and DVT) with COVID-19 is not well understood. Individuals with COVID-19 may have some complex coagulation abnormalities that create a hypercoagulable state but these cannot be recognized unless thrombosis occurs.
Circulating prothrombotic factors have been reported or suggested in patients with severe COVID-19 including elevated Factor VIII and fibrinogen levels. Vascular endothelial inflammation and injury may also contribute to the thrombotic tendency.
From a coding perspective, when thrombosis occurs in a patient with a recent COVID-19 infection, coding depends on whether there is an active COVID-19 infection or it has resolved. With an active infection, U07.1, COVID-19, is assigned first followed by all the complications such as the type and location of thrombo-embolism and the underlying hypercoagulable state if documented.
When a hypercoagulable state due to COVID-19 occurs after the active infection has resolved, the reason for admission (e.g., DVT and/or PE) is sequenced first followed by U09.9, post-COVID condition.
According to the CDC, 4.5 million Americans have chronic liver disease and almost 48,000 die from it each year.
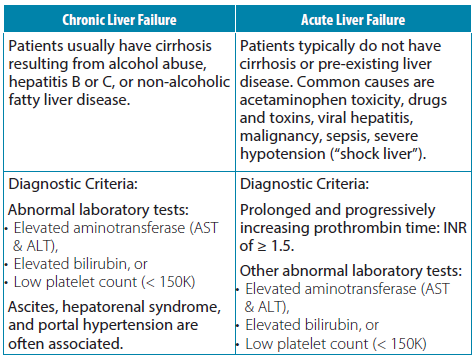
From a coding and CDI perspective, chronic (or unspecified) liver failure is a non-CC and acute liver (hepatic) failure is classified as an MCC. How do we recognize chronic vs. acute liver failure? The table below illustrates the primary differences.
Other laboratory and clinical findings in liver failure include elevated creatinine, amylase/lipase, GGT, alkaline phosphatase, LDH; low pre-albumin/albumin; anemia. Physical findings include jaundice, hepatomegaly, RUQ/liver tenderness, ascites/edema, and asterixis (rhythmic “flapping” of hands when wrists held fully extended).
Get our CDI Pocket Guide® for more help with hepatic encephalopathy and failure.
What is hepatic encephalopathy? Patients with chronic liver failure are often admitted with hepatic encephalopathy which describes a spectrum of neurologic impairment. Symptoms include altered mental status, confusion, disorientation, inappropriate behavior, combativeness, gait disturbances, and/or altered level of consciousness ranging from drowsiness to deep coma. An elevated level of neurotoxic blood ammonia confirms the diagnosis, and it is treated with lactulose. Hepatic encephalopathy can be acute (overt), chronic, or acute on chronic.
From a coding perspective, hepatic encephalopathy does not have its own ICD-10 code and is indexed to “hepatic failure, not elsewhere classified” (category K72). When a patient is admitted with hepatic encephalopathy due to chronic liver cirrhosis, hepatic encephalopathy would be assigned as the principal diagnosis.
Case Studies: Demand Ischemia, Non-Ischemic Myocardial Injury, and Type 2 MI
Case #1: A 66-year-old male is admitted with PAT and substernal chest pressure with ventricular rate of 180. Troponin = 0.01--0.03--0.02 (Ref Range 0.0−0.04). PAT and chest pain resolved with IV Cardizem. Physician diagnosis: (1) PAT and (2) Troponin leak due to supply/demand mismatch.
Answer: This clinically indicates demand ischemia since the troponins were in normal range, but with evidence of acute ischemia (chest pressure). The PAT created a myocardial oxygen demand that exceeded myocardial oxygen supply.
Demand ischemia describes myocardial ischemia primarily due to cardiac supply/demand mismatch rather than CAD. In other words, the supply of blood flow to the heart is not limited but is inadequate to match the increased oxygen demands of an increased workload on the heart. Supply/demand ischemia can be either “demand ischemia” (no infarction) or “Type 2 MI” (infarction due to supply/demand mismatch). Because the troponins were within the normal range, this would not be classified as a Type 2 myocardial infarction.
Case #2: A 62-year-old male with a personal medical history of CHF, myocardial infarction, CAD with three stents, ischemic cardiomyopathy, and CKD, is admitted for acutely decompensated chronic systolic CHF. He had no chest pain or other ischemic symptoms. The initial troponin level was 0.26 (URL <0.10) which slowly trended downward: 0.19, 0.15, 0.14. EKG reported ST and T-wave abnormality, consider inferolateral ischemia.
The attending physician spoke with Cardiology who believed the troponin elevation was likely due to a combination of CKD and “troponin leak” from cardiac strain due to CHF. The attending MD documented Troponin above reference range. No further testing was done.
Answer: This clinically indicates non-ischemic myocardial injury. Although there were positive troponins, they were relatively flat, and the cardiologist indicated that the troponin elevation is likely due to non-ischemic causes - a combination of CKD and “troponin leak” from cardiac strain due to CHF. CHF and CKD are common "non-ischemic" causes of elevated troponins, and there was no further testing or treatment for the patient's CAD. There is also nothing stated in the record to indicate symptoms of ischemia, the EKG report notwithstanding. Non-ischemic causes of troponin elevation may be cardiac or non-cardiac in origin.
Case #3: An 82-year-old male admitted with BP 250/135, neck and shoulder pain and shortness of breath. EKG reported NSTTW changes. Troponin = 0.08--1.5--1.8. (Ref Range 0.00−0.04). BP reduced to 160/90 with IV nitroglycerin. Also given aspirin, atenolol, ASA, and clopidogrel. Repeat EKG prior to discharge unchanged.
Discharge Diagnosis: (1) Hypertensive emergency, and (2) NSTEMI probably due to #1 – prob demand ischemia.
Answer: This clinically supports a Type 2 MI based on the elevated Troponins above the 99th percentile with a rise and/or fall, and evidence of acute ischemia with neck and shoulder pain and shortness of breath, as well as EKG changes. The cause was hypertensive emergency, and not CAD. A type 1 NSTEMI is due to CAD.
Based on discharge diagnosis, this must be coded as a Type 2 MI. According to official coding guidelines, a "NSTEMI probably due to demand ischemia" is assigned to code I21.A1, Myocardial infarction type 2 with the underlying cause coded first.
Get our CDI Pocket Guide to learn more about myocardial ischemia, injury and infarction.
COVID-19: Is it current or resolved? (Timing is everything!)
We have learned much about COVID-19 since the pandemic began a year ago. We have new and better treatments, better patient outcomes, and better understanding of the complications and long-lasting effects of this coronavirus. New coding guidelines have been developed, with a new ICD-10 code (U07.1), and the guidelines continue to evolve.
Because the U07.1 code can substantially affect hospital reimbursement, audit contractors are paying very close attention. In this post we want to shed light on the most important factor in accurate coding and DRG assignment for COVID-19, which is the distinction between an active infection and one that is considered resolved.
We begin with the Official Coding Guidelines, which states that only confirmed cases of COVID-19 are coded U07.1. A confirmed case is defined as having either:
1. A positive COVID-19 test result
or
2. Provider documentation that the individual has COVID-19.
This definition accounts for the fact that the standard PCR and point-of-service rapid antigen tests for COVID-19 are reliable when positive but not so much when "negative." A negative result does not rule out COVID19, because the window of time in which these tests can detect the virus is very limited (it must still be detectable in the upper respiratory tract). These false negative rates range from 20% to 60% depending on whether the patient has symptoms. Therefore, the provider can make a clinical decision whether the patient has COVID-19 infection, even if the test is negative or no test was performed.
How are hospitals reimbursed for COVID-19?
Hospitals are reimbursed for COVID-19 patients based on the assignment of ICD-10 code U07.1 on a claim. The hospital also earns an extra 20% bonus from CMS to cover the unusual costs of treating and isolating an infectious patient in a pandemic.
If U07.1 is coded as the principal diagnosis, the following DRGs might be assigned: DRG 177-179 (Respiratory Infections), DRGs 207-208 (with ventilator), and sometimes DRGs 981-983/987-989 if an OR procedure is performed.
If code U07.1 is assigned as a secondary diagnosis, it is classified as an MCC—even if the patient is asymptomatic.
What criteria must be met for the 20% bonus?
Because testing strategies have evolved, and a 20% bonus is something payers will not eagerly part with, the rules changed as of September 1, 2020. Now, to qualify for the 20% reimbursement bonus, the record must contain a positive COVID-19 test (either during the admission or within 14 days prior to admission). If the record does not contain the positive test report, hospitals can decline the additional payment at the time of claim submission to avoid repayment.
When is it appropriate to code U07.1?
According to current coding guidelines, code U07.1 can be assigned for patients admitted with a positive COVID test or manifesting an active infection.
Patients readmitted with complications or residual effects of a previous COVID-19 infection are not coded with U07.1, because their infection is considered to be inactive or have "resolved." Symptoms can linger, evolve, or rebound, but these do not prove that the virus is still active or infectious.
How do we know if a patient’s COVID-19 infection has resolved?
In short, we can't know for sure, but there are guidelines.
The CDC states that “Available data indicate that persons with mild to moderate COVID-19 remain infectious no longer than 10 days after symptom onset. Persons with more severe to critical illness or severe immunocompromise likely remain infectious no longer than 20 days after symptom onset; however, there have been several reports of people shedding replication-competent virus beyond 20 days due to severe immunocompromise."
So, if the patient has mild to moderate COVID-19, they're considered resolved after 10 days from onset.
If the patient has severe or critical illness, or is immunocompromised, the infection may be active up to 20 days from onset.
There are also clinical clues that an infection has resolved: the patient isn't isolated, and there is no COVID-19 treatment being given (remdesivir, decadron/dexamethasone, etc.).
The trouble with retesting
Although a repeat test may be useful in patients with new symptoms, retesting is not generally recommended, because patients who have recovered from a COVID-19 infection may continue to shed viral RNA or dead virus may continue to circulate in the body. True reinfection is uncommon. Therefore, the CDC advises that providers not repeat COVID tests following an initial positive test.
Whether or not COVID-19 is assigned as the principal diagnosisis dependent on whether the COVID-19 infection has resolved which is determined by provider documentation. If a patient is admitted with a residual effect (sequelae) and the provider documentation indicates the COVID-19 infection has resolved or the patient is no longer infectious (even with a current or recent positive COVID-19 test), assign a code for the residual effect as principal diagnosis and code U09.9, Post-COVID-19 condition. If the COVID-19 infection has not resolved, assign code U07.1 as principal diagnosis and the manifestation as a secondary diagnosis.
Coding Clinic 2021 Fourth Quarter has clarified that even if a patient has a current or recent positive test for COVID-19, when provider documentation indicates that a patient is not actively infectious during the admission, this indicates that the patient no longer has an active COVID-19 infection, and code U07.1 would not be assigned. See FAQ pages 21-24, Questions #53, 55-58.
Best practice recommendations
Considering the CDC data and the CMS requirement for a positive test within the past 14 days, a good rule of thumb is that if it's been more than 14 days since a patient had onset of mild or moderate symptoms, or more than 20 days in a severely ill patient, then the infection is likely to have resolved.
Based on official coding guidelines and the ICD-10-CM instructions for COVID-19, the following are six clinical and coding scenarios to help guide you in coding and sequencing code U07.1.
Example cases: Test your coding skills!
Case 1. Patient admitted with pneumonia and respiratory failure. Patient tested positive for COVID-19 infection 10 days ago.
Here, Code U07.1 is assigned as the principal diagnosis, with the respiratory manifestations as secondary diagnoses. According to Coding Clinic, providers do not have to explicitly link the respiratory manifestation with COVID-19 since the causal relationship is implied. Common respiratory manifestations include pneumonia, lower respiratory infection, pneumothorax, acute respiratory failure, and ARDS. The test report should be accessed and included in the admission record.
Case 2. A patient was diagnosed with COVID-19 infection a week ago and is admitted after developing acute shortness of breath associated with upper back pain as well as dizziness, fever and cough. The patient was discharged with the diagnosis of pulmonary embolism (PE) due to COVID-19 infection.
When the reason for the admission is a non-respiratory manifestation of COVID-19, code U07.1 is assigned as the principal diagnosis and the manifestation(s) as secondary. In applying this rule, the provider must specifically “link” COVID and a non-respiratory manifestation. Common non-respiratory manifestations include thrombo-embolism resulting in CVA, MI, DVT, pulmonary embolism; COVID-related enteritis, multisystem inflammatory syndrome in children (MIS-C), cytokine release syndrome, and Guillain-Barré syndrome. Here, pulmonary embolism is assigned as a secondary diagnosis.
Case 3. Patient was admitted with COVID-19 pneumonia three weeks ago, and is now being readmitted for a pulmonary embolism.
This is a great example of coding the sequelae of COVID-19. A sequela is a manifestation or complication of a previous condition (sequelae is the plural). When a patient is admitted with sequela of a prior COVID-19 infection, code the sequela as the principal diagnosis with a secondary diagnosis code of U09.9, Post-COVID condition. Some common sequelae include pneumonia, cytokine release syndrome, thromboembolism resulting in CVA, MI, DVT or PE and heart failure (for those who had COVID myocarditis).
In this case, since it's been three weeks since the last admission (and therefore > 14 days since symptom onset), we would assign pulmonary embolism as the principal diagnosis, and U09.9 as a secondary diagnosis.
Case 4. Elderly patient was admitted for hip fracture s/p fall at home. Patient has weakness and generalized debility due to prolonged hospitalization one month ago for COVID-19.
Here the patient has a hip fracture, which is not directly related to the previous COVID-19 infection, which has resolved by now. We would assign the unrelated condition (hip fracture) as the principal diagnosis and assign code Z86.16 (Personal history of COVID-19) as a secondary diagnosis. Personal history codes account for a patient's past medical condition that no longer exists and is not being treated but may recur. According to Coding Clinic, code U09.9 (sequelae) would not be assigned, as the debility is due to the prolonged hospitalization rather than COVID-19 infection itself.
Case 5. Patient admitted with severe anemia due to chronic GI bleeding. Also experienced low-grade fever and mild shortness of breath, which led the hospital to test for COVID-19. The patient tested positive, was placed in isolation, and treated with blood transfusions.
When an admitted patient has COVID-19 and an unrelated condition, sequencing depends on which diagnosis meets the definition of the principal diagnosis. When two or more diagnoses "equally meet the criteria for principal diagnosis as determined by the circumstances of admission, diagnostic workup, and/or therapy provided ….any one of the diagnoses may be sequenced first.”
The circumstances in this case favor anemia as the focus of admission, particularly since COVID-19 in this case was not severe enough to require admission on its own. Assign anemia as principal diagnosis and COVID-19 (U07.1) as secondary diagnosis.
Special cases: Sepsis, Transplant Complications, and Obstetrics
In these special cases, code U07.1 follows the required principal diagnosis definition based on Official Coding Guidelines:
Case 6. Patient is admitted with COVID pneumonia and sepsis. Whether or not sepsis or U07.1 is assigned as the principal diagnosis depends on the circumstances of admission and whether sepsis meets the definition of principal diagnosis. For example, if a patient is admitted with pneumonia due to COVID-19 which then progresses to viral sepsis (not present on admission), the principal diagnosis is U07.1, COVID-19, followed by the codes for the viral sepsis and viral pneumonia. On the other hand, if a patient is admitted with sepsis due to COVID-19 pneumonia and sepsismeets the definition of principal diagnosis, then the code for viral sepsis (A41.89) would be assigned as principal diagnosis followed by codes U07.1 and J12.82, as secondary diagnoses. In most cases, the principal reason for admission and focus of treatment is the COVID-19 pneumonia and its consequences, with U07.1 assigned as the principal diagnosis.
Case 7. Patient is status post lung transplant, admitted with pneumonia and COVID-19. The transplant complication code (T86.812) is assigned as principal diagnosis since the pneumonia is affecting the function of the transplanted organ.
Case 8. A patient who is 30 weeks pregnant is admitted with COVID-19. Code O98.5 (Other viral diseases complicating pregnancy, childbirth and the puerperium), is assigned as the principal diagnosis and code U07.1 with the associated manifestation(s) are secondary diagnoses.
When should we query?
Physicians and other healthcare staff are overwhelmed with high caseloads of very sick COVID-19 patients. Therefore, although hospitals should use code U07.1 when it is appropriate, we also want to minimize COVID-19 queries.
CDI and coding specialists should consider the above “rule of thumb” when patients are admitted with a previous COVID-19 infection (“history of,” “convalesced,” "resolved”). In many of these situations, no query would be needed and code U07.1 would not be assigned—even if the patient continues to test positive.
If there are indicators of a current, active infection, such as 14 days or less since COVID-19 infection (or positive test), treatment with medications for COVID-19 (dexamethasone, remdesivir, etc.), or the patient is placed in isolation, then a query would likely be productive if the documentation is unclear.
Other situations when a query may be needed is when provider documentation is unclear whether a non-respiratory condition is related to a current COVID-19 infection. Clinical validation comes into play when clinical indicators are questionable and test results are negative or absent; pay attention to the combination of duration since symptom onset and severity of symptoms—remember, severe cases or people who are immunocompromised may have active infections up to 20 days from onset, rather than 10 days for less severe cases.
Updated 02/07/2022 with new ICD-10 codes.
MS-DRG Tables 2008 through 2022
Find all CMS MS-DRG Tables for FY2008 through FY2022 in the link below.
What is clinical validation? Why is it important? What’s the big deal? Is it not enough to just query the provider?
Clinical validation is the process of validating each diagnosis or procedure documented within the health record, ensuring it is supported by clinical evidence in the medical record. Based on the False Claims Act of 1863, CMS does not permit providers to submit claims with codes for conditions that cannot be clinically validated based on authoritative and/or widely accepted diagnostic standards if it results in an “overpayment.”
Penalties can be severe. Please be reassured that the organization is “at risk”, not its employees so long as they follow the hospital’s policy.
Claim submission and reimbursement are governed by CMS regulations and policy manuals including the RAC Statement of Work which require clinical validation of diagnoses submitted on claims. Everyone is aware that clinical validity is a primary focus of Medicare Advantage and commercial payers, and clinical validation is the most frequent reason for DRG payment reductions.
CMS RAC Statement of Work
CMS Medicare Program Integrity Manual
False Claims Act of 1863
“Clinical validation involves a clinical review of the case to see whether or not the patient truly possesses the conditions that were documented in the medical record.”
“The purpose of DRG validation is to ensure that diagnostic and procedural information…coded and reported by the hospital on its claims matches the attending physician’s description and the information contained in the medical record.”
Imposes civil liability on any person (or organizations) who knowingly submits, or causes the submission of, a false or fraudulent claim to the Federal government. “Knowingly” is actual knowledge, deliberate ignorance, or reckless disregard. Includes submitting a claim with a higher weighted DRG than supported by the medical record.
The consequences of submitting clinically invalid diagnoses are numerous: improper DRG reimbursement, excessive denials, unnecessary appeals, risk of regulatory audits and penalties. Over-coding leads to MCC/CC classification downgrades, as have occurred with AKI and encephalopathy. To add insult to injury, denials and appeals mostly serve to enrich audit contractors at the expense of the Medicare trust fund.
Get our CDI Pocket Guide® for more help with clinical validation.
How we ensure compliance with these statutory and regulatory imperatives has become controversial, if not contentious. Some argue that the provider’s diagnostic statement is enough for code assignment relying on the Official Coding Guidelines (OCG) Section I.A.19 statement since 2016 that:
“The assignment of a diagnosis code is based on the provider’s diagnostic statement that the condition exists. The provider’s statement that the patient has a particular condition is sufficient. Code assignment is not based on clinical criteria used by the provider to establish the diagnosis.”
We are caught between an irreconcilable CMS requirement for compliant submission of claims and reimbursement and the Official Guidelines for Coding and Reporting.
What is to be done? Many argue that a clinical validation query to the provider is enough, relying on his response to decide whether to assign a code for the condition. A request for additional clinical information substantiating the diagnosis is recommended.
What if the provider doesn’t respond or additional clinical information is not provided? We still haven’t escaped the CMS claims submission requirement for which both the clinician and hospital are responsible, and we therefore cannot include the code on the claim. What would you prefer, non-compliant billing and reimbursement with potentially severe consequences or deciding to omit the code as directed by CMS for which there are no consequences?
Each organization must have its own policy for dealing with these clinical validation issues taking into consideration the relative consequences. When diagnoses are obviously invalid, the CDI team – coding, clinical documentation specialists, physician advisor – is certainly qualified to make a decision to omit a code. After all, there are no consequences for removing a clinically invalid diagnosis code but more serious problems if you don't.